
 It affects mainly older individuals, and is associated with obesity, hypothyroidism, diabetes, pregnancy, family history, rheumatoid arthritis, and wrist shape. In spite of common feelings otherwise, there is very limited relation between work-related repetitive motion and carpal tunnel syndrome. The cause of the syndrome is a compression of the carpal tunnel, causing an impingement on the median nerve of the wrist. This causes pain or numbness in the fingers and thumb. The carpal tunnel release procedure involves reducing this impingement by cutting the carpal ligament. Then, after removing any enlarged tissue surrounding the median nerve, the carpal ligament is lengthened and reattached. The surgery is done on an outpatient basis and usually usually takes about a week of rest before beginning a rehabilitation program to regain muscle control. Results are usually very good, with complete reduction of pain and full mobility retained. This is one of the most common procedures performed by orthopedic surgeons in the United States.
It affects mainly older individuals, and is associated with obesity, hypothyroidism, diabetes, pregnancy, family history, rheumatoid arthritis, and wrist shape. In spite of common feelings otherwise, there is very limited relation between work-related repetitive motion and carpal tunnel syndrome. The cause of the syndrome is a compression of the carpal tunnel, causing an impingement on the median nerve of the wrist. This causes pain or numbness in the fingers and thumb. The carpal tunnel release procedure involves reducing this impingement by cutting the carpal ligament. Then, after removing any enlarged tissue surrounding the median nerve, the carpal ligament is lengthened and reattached. The surgery is done on an outpatient basis and usually usually takes about a week of rest before beginning a rehabilitation program to regain muscle control. Results are usually very good, with complete reduction of pain and full mobility retained. This is one of the most common procedures performed by orthopedic surgeons in the United States.
4/3/09
Procedure Profile: Carpal Tunnel Release
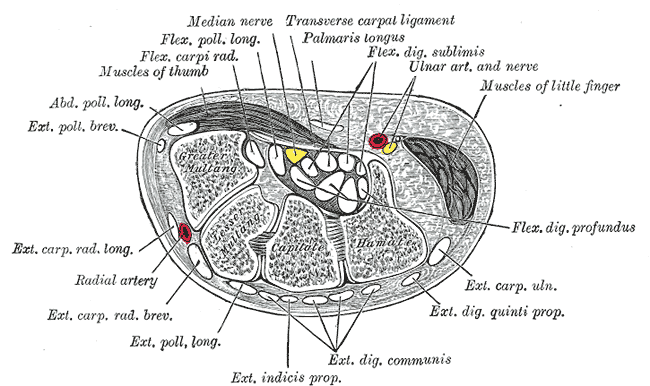
Carpal tunnel syndrome is fairly common in our population today.  It affects mainly older individuals, and is associated with obesity, hypothyroidism, diabetes, pregnancy, family history, rheumatoid arthritis, and wrist shape. In spite of common feelings otherwise, there is very limited relation between work-related repetitive motion and carpal tunnel syndrome. The cause of the syndrome is a compression of the carpal tunnel, causing an impingement on the median nerve of the wrist. This causes pain or numbness in the fingers and thumb. The carpal tunnel release procedure involves reducing this impingement by cutting the carpal ligament. Then, after removing any enlarged tissue surrounding the median nerve, the carpal ligament is lengthened and reattached. The surgery is done on an outpatient basis and usually usually takes about a week of rest before beginning a rehabilitation program to regain muscle control. Results are usually very good, with complete reduction of pain and full mobility retained. This is one of the most common procedures performed by orthopedic surgeons in the United States.
It affects mainly older individuals, and is associated with obesity, hypothyroidism, diabetes, pregnancy, family history, rheumatoid arthritis, and wrist shape. In spite of common feelings otherwise, there is very limited relation between work-related repetitive motion and carpal tunnel syndrome. The cause of the syndrome is a compression of the carpal tunnel, causing an impingement on the median nerve of the wrist. This causes pain or numbness in the fingers and thumb. The carpal tunnel release procedure involves reducing this impingement by cutting the carpal ligament. Then, after removing any enlarged tissue surrounding the median nerve, the carpal ligament is lengthened and reattached. The surgery is done on an outpatient basis and usually usually takes about a week of rest before beginning a rehabilitation program to regain muscle control. Results are usually very good, with complete reduction of pain and full mobility retained. This is one of the most common procedures performed by orthopedic surgeons in the United States.
It affects mainly older individuals, and is associated with obesity, hypothyroidism, diabetes, pregnancy, family history, rheumatoid arthritis, and wrist shape. In spite of common feelings otherwise, there is very limited relation between work-related repetitive motion and carpal tunnel syndrome. The cause of the syndrome is a compression of the carpal tunnel, causing an impingement on the median nerve of the wrist. This causes pain or numbness in the fingers and thumb. The carpal tunnel release procedure involves reducing this impingement by cutting the carpal ligament. Then, after removing any enlarged tissue surrounding the median nerve, the carpal ligament is lengthened and reattached. The surgery is done on an outpatient basis and usually usually takes about a week of rest before beginning a rehabilitation program to regain muscle control. Results are usually very good, with complete reduction of pain and full mobility retained. This is one of the most common procedures performed by orthopedic surgeons in the United States.
4/1/09
Tendon Transfer Surgery - Ingenuity solves life's most difficult situations
This post is related more directly to the surgery aspect of my blog, as opposed to the most recent posts which had been more concerned with aging and frailty.  As mentioned in the title, I would like to cover the procedure of tendon transfer surgery. Just as the name implies, it involves the relocation of a tendon from one muscle to a bone that was previously moved by another muscle. This is practical to do for a quadriplegic patient who has retained movement of the shoulders but has lost control of the arms and hands. This situation is fairly common as the nerves running to the shoulder do not pass through the spinal cord with the rest of the nerves or the lower body. Therefore, an injury even to the highest level of the spinal cord frequently spares the shoulder nerves. Thus, the controllable trapezius muscle is partially removed from the shoulder and reattached lower on the arm or in the hand or thumb to provide either wrist movement, arm movement, or pinching ability. While the possibilities for transplant are limited, the results are a gift for those who receive the surgery. Quality of life goes up dramatically due to increased independence. This procedure is amazing in it's inherent simplicity (just move the attachment point of a muscle to provide a new function) and there is true beauty in its outcome.
As mentioned in the title, I would like to cover the procedure of tendon transfer surgery. Just as the name implies, it involves the relocation of a tendon from one muscle to a bone that was previously moved by another muscle. This is practical to do for a quadriplegic patient who has retained movement of the shoulders but has lost control of the arms and hands. This situation is fairly common as the nerves running to the shoulder do not pass through the spinal cord with the rest of the nerves or the lower body. Therefore, an injury even to the highest level of the spinal cord frequently spares the shoulder nerves. Thus, the controllable trapezius muscle is partially removed from the shoulder and reattached lower on the arm or in the hand or thumb to provide either wrist movement, arm movement, or pinching ability. While the possibilities for transplant are limited, the results are a gift for those who receive the surgery. Quality of life goes up dramatically due to increased independence. This procedure is amazing in it's inherent simplicity (just move the attachment point of a muscle to provide a new function) and there is true beauty in its outcome.
 As mentioned in the title, I would like to cover the procedure of tendon transfer surgery. Just as the name implies, it involves the relocation of a tendon from one muscle to a bone that was previously moved by another muscle. This is practical to do for a quadriplegic patient who has retained movement of the shoulders but has lost control of the arms and hands. This situation is fairly common as the nerves running to the shoulder do not pass through the spinal cord with the rest of the nerves or the lower body. Therefore, an injury even to the highest level of the spinal cord frequently spares the shoulder nerves. Thus, the controllable trapezius muscle is partially removed from the shoulder and reattached lower on the arm or in the hand or thumb to provide either wrist movement, arm movement, or pinching ability. While the possibilities for transplant are limited, the results are a gift for those who receive the surgery. Quality of life goes up dramatically due to increased independence. This procedure is amazing in it's inherent simplicity (just move the attachment point of a muscle to provide a new function) and there is true beauty in its outcome.
As mentioned in the title, I would like to cover the procedure of tendon transfer surgery. Just as the name implies, it involves the relocation of a tendon from one muscle to a bone that was previously moved by another muscle. This is practical to do for a quadriplegic patient who has retained movement of the shoulders but has lost control of the arms and hands. This situation is fairly common as the nerves running to the shoulder do not pass through the spinal cord with the rest of the nerves or the lower body. Therefore, an injury even to the highest level of the spinal cord frequently spares the shoulder nerves. Thus, the controllable trapezius muscle is partially removed from the shoulder and reattached lower on the arm or in the hand or thumb to provide either wrist movement, arm movement, or pinching ability. While the possibilities for transplant are limited, the results are a gift for those who receive the surgery. Quality of life goes up dramatically due to increased independence. This procedure is amazing in it's inherent simplicity (just move the attachment point of a muscle to provide a new function) and there is true beauty in its outcome.
3/29/09
Exercise and Longevity
As I mentioned in my previous posts here and here, exercise can be beneficial to older adults for a number of reasons.  Exercise is perhaps one of the most important weapons in the fight against aging because of its myriad of positive effects on the body. This paper summarizes the results from a number of studies and concludes that regular aerobic exercise an increase mood, energy levels, strength, balance, and coordination. This sounds remarkably like the effects of HGH supplementation. In addition to these immediate effects, regular exercisers also had lower overall death rates than their sedentary counterparts. In fact, the individuals in any given age group (accounting for gender) with the lowest death rates were also the most active. In addition to even this is the increased independence for older adults who exercise regularly. Being physically fit can decrease the chances of a fall, and reduce the effects of one on the body. Stronger bones are more resistant to fracture, after all. The National Acadamie's Institute of Medicine suggests that all Americans aim for 60 minutes of physical activity each day.
Exercise is perhaps one of the most important weapons in the fight against aging because of its myriad of positive effects on the body. This paper summarizes the results from a number of studies and concludes that regular aerobic exercise an increase mood, energy levels, strength, balance, and coordination. This sounds remarkably like the effects of HGH supplementation. In addition to these immediate effects, regular exercisers also had lower overall death rates than their sedentary counterparts. In fact, the individuals in any given age group (accounting for gender) with the lowest death rates were also the most active. In addition to even this is the increased independence for older adults who exercise regularly. Being physically fit can decrease the chances of a fall, and reduce the effects of one on the body. Stronger bones are more resistant to fracture, after all. The National Acadamie's Institute of Medicine suggests that all Americans aim for 60 minutes of physical activity each day.
 Exercise is perhaps one of the most important weapons in the fight against aging because of its myriad of positive effects on the body. This paper summarizes the results from a number of studies and concludes that regular aerobic exercise an increase mood, energy levels, strength, balance, and coordination. This sounds remarkably like the effects of HGH supplementation. In addition to these immediate effects, regular exercisers also had lower overall death rates than their sedentary counterparts. In fact, the individuals in any given age group (accounting for gender) with the lowest death rates were also the most active. In addition to even this is the increased independence for older adults who exercise regularly. Being physically fit can decrease the chances of a fall, and reduce the effects of one on the body. Stronger bones are more resistant to fracture, after all. The National Acadamie's Institute of Medicine suggests that all Americans aim for 60 minutes of physical activity each day.
Exercise is perhaps one of the most important weapons in the fight against aging because of its myriad of positive effects on the body. This paper summarizes the results from a number of studies and concludes that regular aerobic exercise an increase mood, energy levels, strength, balance, and coordination. This sounds remarkably like the effects of HGH supplementation. In addition to these immediate effects, regular exercisers also had lower overall death rates than their sedentary counterparts. In fact, the individuals in any given age group (accounting for gender) with the lowest death rates were also the most active. In addition to even this is the increased independence for older adults who exercise regularly. Being physically fit can decrease the chances of a fall, and reduce the effects of one on the body. Stronger bones are more resistant to fracture, after all. The National Acadamie's Institute of Medicine suggests that all Americans aim for 60 minutes of physical activity each day.
3/27/09
Capromorelin - New Drug to Prevent Frailty in Old Age?
The American pharmaceutical giant Pfizer has recently released a new drug that holds promise to reduce the effects of aging. Capromorelin has been shown to increase levels of human growth hormone in elderly patients. The effects of this increase in HGH include lean muscle gain, improved balance, and improved coordination. Human growth hormone levels typically peak from late childhood to around puberty, when growth is most rapid. From then on, levels decline steadily and then drop off quickly after about age sixty. This decrease is associated with a lack of energy, less powerful immune system, and more rapid 'wear and tear' on the body. Theoretically, bringing HGH levels back up to near-puberty levels could bring back some youthful vigor to an otherwise frail individual. While this may be the case, it is also possible to raise HGH levels naturally through exercise, proper diet, and adequate sleep. For the time being, these may be safer options for healthy people considering a drug to increase their growth hormone production.
3/26/09
Osteoporsis - Preventative Measures
One of the leading causes of debilitation of women over the age of 50 in the United States is osteoporosis.  Bones are constantly being broken down and rebuilt by osteoclasts and osteoblasts, respectively. This process is known as bone remodeling. Osteoporosis is condition in which bones are destroyed at a rate faster than they are rebuilt and therefore become weaker over time. Since an increase in osteoclast activity can lead to a reduction in bone mass, it has been proposed that estrogen (which stimulates osteoblast activity) could be used to combat the effects of osteoporosis. This theory also explains why osteoporosis affects primarily post-menopausal women (women who are producing less estrogen than they previously were).
Bones are constantly being broken down and rebuilt by osteoclasts and osteoblasts, respectively. This process is known as bone remodeling. Osteoporosis is condition in which bones are destroyed at a rate faster than they are rebuilt and therefore become weaker over time. Since an increase in osteoclast activity can lead to a reduction in bone mass, it has been proposed that estrogen (which stimulates osteoblast activity) could be used to combat the effects of osteoporosis. This theory also explains why osteoporosis affects primarily post-menopausal women (women who are producing less estrogen than they previously were).
Preventing osteoporosis is a worthy goal, and there are several ways to go about it. First and most importantly is calcium intake. Calcium in the bloodstream is necessary for both slowing bone breakdown and promoting bone formation. Increasing dietary calcium can lead to this desired effect. Secondly, vitamin D is needed to promote absorption of calcium. Vitamin D can be absorbed through the skin from sunlight, and can also be ingested. Vitamin D fortified milk is an excellent source of both calcium and vitamin D.
Finally, exercise is a great way to slow osteoporosis. Bones respond to stress by building more bone. Running, for example, will help strengthen the bones of the lower body and help prevent the onset of frailty. It is important to note that impact exercies should be undertaken gradually in order to reduce the risk of developing stress fractures in individuals who already are experiencing some early form of osteoporosis.
 Bones are constantly being broken down and rebuilt by osteoclasts and osteoblasts, respectively. This process is known as bone remodeling. Osteoporosis is condition in which bones are destroyed at a rate faster than they are rebuilt and therefore become weaker over time. Since an increase in osteoclast activity can lead to a reduction in bone mass, it has been proposed that estrogen (which stimulates osteoblast activity) could be used to combat the effects of osteoporosis. This theory also explains why osteoporosis affects primarily post-menopausal women (women who are producing less estrogen than they previously were).
Bones are constantly being broken down and rebuilt by osteoclasts and osteoblasts, respectively. This process is known as bone remodeling. Osteoporosis is condition in which bones are destroyed at a rate faster than they are rebuilt and therefore become weaker over time. Since an increase in osteoclast activity can lead to a reduction in bone mass, it has been proposed that estrogen (which stimulates osteoblast activity) could be used to combat the effects of osteoporosis. This theory also explains why osteoporosis affects primarily post-menopausal women (women who are producing less estrogen than they previously were).Preventing osteoporosis is a worthy goal, and there are several ways to go about it. First and most importantly is calcium intake. Calcium in the bloodstream is necessary for both slowing bone breakdown and promoting bone formation. Increasing dietary calcium can lead to this desired effect. Secondly, vitamin D is needed to promote absorption of calcium. Vitamin D can be absorbed through the skin from sunlight, and can also be ingested. Vitamin D fortified milk is an excellent source of both calcium and vitamin D.
Finally, exercise is a great way to slow osteoporosis. Bones respond to stress by building more bone. Running, for example, will help strengthen the bones of the lower body and help prevent the onset of frailty. It is important to note that impact exercies should be undertaken gradually in order to reduce the risk of developing stress fractures in individuals who already are experiencing some early form of osteoporosis.
3/22/09
Assistive Technology for Older Americans
While this may not be directly related to orthopedic surgery, I feel that I should discuss the current situation of assistive technologies for older adults. This is because older adults are a large (and growing) population that is prone to conditions that sometimes warrant surgery and other times require technological assistance, such as a mobile scooter or a walker. These kinds of technologies can be crucial in maintaining a senior citizen's mobility and independence, but they are not cheap. It can be difficult for an individual to afford these items, or other more expensive technologies like modified bathrooms, and there is limited funding available to help support these cases. According to the Executive Director of the American Society on Aging, Gloria Cavanaugh, the major hurdle is often proving that these devices or home modifications are 'medically necessary.' Healthcare providers are often hesitant to approve funding for assistive technologies, since they claim that they are essentially frivolous. The fact of the matter though, is that these assistive technologies can dramatically improve the quality of life for an older individual by preserving independence and eliminating the need for a personal caretaker. This is a great reason to approve funding, in my opinion. One of the most difficult aspects of aging in America is the dependence that is associated with it. Prolonging the independence of a senior citizen should always be a priority.
This is because older adults are a large (and growing) population that is prone to conditions that sometimes warrant surgery and other times require technological assistance, such as a mobile scooter or a walker. These kinds of technologies can be crucial in maintaining a senior citizen's mobility and independence, but they are not cheap. It can be difficult for an individual to afford these items, or other more expensive technologies like modified bathrooms, and there is limited funding available to help support these cases. According to the Executive Director of the American Society on Aging, Gloria Cavanaugh, the major hurdle is often proving that these devices or home modifications are 'medically necessary.' Healthcare providers are often hesitant to approve funding for assistive technologies, since they claim that they are essentially frivolous. The fact of the matter though, is that these assistive technologies can dramatically improve the quality of life for an older individual by preserving independence and eliminating the need for a personal caretaker. This is a great reason to approve funding, in my opinion. One of the most difficult aspects of aging in America is the dependence that is associated with it. Prolonging the independence of a senior citizen should always be a priority.
 This is because older adults are a large (and growing) population that is prone to conditions that sometimes warrant surgery and other times require technological assistance, such as a mobile scooter or a walker. These kinds of technologies can be crucial in maintaining a senior citizen's mobility and independence, but they are not cheap. It can be difficult for an individual to afford these items, or other more expensive technologies like modified bathrooms, and there is limited funding available to help support these cases. According to the Executive Director of the American Society on Aging, Gloria Cavanaugh, the major hurdle is often proving that these devices or home modifications are 'medically necessary.' Healthcare providers are often hesitant to approve funding for assistive technologies, since they claim that they are essentially frivolous. The fact of the matter though, is that these assistive technologies can dramatically improve the quality of life for an older individual by preserving independence and eliminating the need for a personal caretaker. This is a great reason to approve funding, in my opinion. One of the most difficult aspects of aging in America is the dependence that is associated with it. Prolonging the independence of a senior citizen should always be a priority.
This is because older adults are a large (and growing) population that is prone to conditions that sometimes warrant surgery and other times require technological assistance, such as a mobile scooter or a walker. These kinds of technologies can be crucial in maintaining a senior citizen's mobility and independence, but they are not cheap. It can be difficult for an individual to afford these items, or other more expensive technologies like modified bathrooms, and there is limited funding available to help support these cases. According to the Executive Director of the American Society on Aging, Gloria Cavanaugh, the major hurdle is often proving that these devices or home modifications are 'medically necessary.' Healthcare providers are often hesitant to approve funding for assistive technologies, since they claim that they are essentially frivolous. The fact of the matter though, is that these assistive technologies can dramatically improve the quality of life for an older individual by preserving independence and eliminating the need for a personal caretaker. This is a great reason to approve funding, in my opinion. One of the most difficult aspects of aging in America is the dependence that is associated with it. Prolonging the independence of a senior citizen should always be a priority.
2/2/09
Increasing population age = more joint replacements
There's another thing that I should have mentioned in my previous post. According to WebMD, hip replacements are expected to rise 174% in the next 20 years, and knee replacements are expected to rise by as much as 673%. That is an astronomical increase in joint replacement surgeries! This relates back to my previous post, when I talked about the increasingly active lifestyle that today's older generations are living. The knee replacement rates are particularly indicative of this. A total knee replacement is frequently performed on an individual who has been active for a lifetime, and consequently has done damage to the knees. This is unavoidable for many active people. Eventually joints wear out, but luckily we have great replacement technology. Total knee replacements can be expected to last for upwards of twenty years without any significant degradation. Of course, it is always possible for an extremely active and young individual who gets a knee replacement to have a revision later without much hassle.
2/1/09
Changing Population Demographics
One of the most interesting pressures that physicians face today is the issue of an aging population. I decided to look into this phenomenon and I found an interesting site called longevity-science.org that talked about this very issue. According to some scholarly predictions, the world's elderly population is expected to rise from 6.9% of the total population today up to 19% by 2050. That is a striking increase, and one that will surely be felt by the medical profession. Orthopedic surgeons will be seeing more joint replacement patients in the years to come since there will be a greater number of elderly individuals leading increasingly active lifestyles. It almost seems improper to refer to today's elderly population as "elderly," considering how physically capable and full of life many of them are. I think it will be great to watch the progression that will take place in the next fifty years. Eventually it will be commonplace to run into centegenarians jogging in the park or lifting weights in the gym. Maybe I'll be lucky enough to be one of them.
1/24/09
Back in the Game
Well, after taking almost a year off from working on the site, I've decided to get back into it all and try to get the Bone Breaker bigger than ever. Look for new posts and research coming soon.
4/14/08
Interactivity and Web 2.0: Getting in touch with other bloggers
This week I again went through the blogosphere in search of quality orthopedic blogs. Thanks to Google Directory, I was able to find two such excellent blogs. The first, Doctor Tarlow on Knees, is maintained by Dr. Stephan Tarlow, an orthopedic surgeon from Scottsdale, Arizona. One of the more recent posts on this blog talked about a new computer program that might be able to help surgeons align replacement knees with greater accuracy. I had a few clarification questions to ask Dr. Tarlow, and the full text of my comment is available below.
The second blog that I found myself reading is actually About.com’s section on orthopedics. I read an interesting post about minimally invasive procedures, and decided to share my opinion with the author, Dr. Jonathan Cluett. Again, the full text of my comment can be found below.
“Otis Med: Shape Matching Custom Fit Total Knee Replacement”
Comment:
Dr. Tarlow,
Very interesting post. I just recently stumbled upon your blog, so let me begin by saying that I am very grateful to read the thoughts of a surgeon who clearly cares very much about providing the best, and sometimes newest treatments for his patients. I am currently an undergrad at the University of Southern California and I am very interested in pursuing a career in surgery, particularly orthopedics.
 So as for your post, I have a few questions regarding knee replacement surgery. You mentioned in your post that in a traditional replacement, the knee is aligned with its axis perpendicular to a line running from hip to ankle. Is a normal knee not always aligned like this? As far as I understood, this is the driving concept behind the Otis Med system, but it seems to me that most knees ought to be pretty close to this ideal that is used in the traditional replacement. In other words, is “customization” really worth the two or three degrees that a patient’s knee may be off by? As you said, the majority of traditional knee replacements can be expected to last several decades.
So as for your post, I have a few questions regarding knee replacement surgery. You mentioned in your post that in a traditional replacement, the knee is aligned with its axis perpendicular to a line running from hip to ankle. Is a normal knee not always aligned like this? As far as I understood, this is the driving concept behind the Otis Med system, but it seems to me that most knees ought to be pretty close to this ideal that is used in the traditional replacement. In other words, is “customization” really worth the two or three degrees that a patient’s knee may be off by? As you said, the majority of traditional knee replacements can be expected to last several decades.
Additionally, why is it that the Otis Med system looks at the degenerated knee and tries to reconstruct it to pick a replacement? Wouldn't it be easier to look at the healthy knee and assume symmetry? That way, no computer reconstruction would be necessary.
Forgive me if my comments seem uninformed or off-base. This is all very interesting to me, so I'm just trying to understand as much as I can.
Thanks,
JDM
“Are surgeries done through small incisions better?”
Comment:
Dr. Cluett,
This is a topic that has interested me for quite some time now. It seems to me that surgeons are constantly on the look out for ways to do less and less invasive surgery. In fact, I have even read about natural-orifice surgeries being performed on patients who really don't want scars. But what intrigues me the most is that often times these minimally invasive surgeries (particularly orthopedic ones, it seems) are very difficult for surgeons to perform, and thus increase the risk of surgical error. Do you think that this is indeed the case? Take, for example, a mini-hip replacement. I have read that there is concern about the ultimate alignment of the prosthesis with this technique.
Other minimally invasive surgeries, though, I feel are done because of a greater understanding of human anatomy. The Quad-sparing knee replacement provides an excellent. This procedure works around the quadriceps instead of through it so that the new joint can be better stabilized post-op. I think that it should be reasons like this, not cosmetic ones, that lead surgeons to create new surgical techniques. Thoughts?
The second blog that I found myself reading is actually About.com’s section on orthopedics. I read an interesting post about minimally invasive procedures, and decided to share my opinion with the author, Dr. Jonathan Cluett. Again, the full text of my comment can be found below.
“Otis Med: Shape Matching Custom Fit Total Knee Replacement”
Comment:
Dr. Tarlow,
Very interesting post. I just recently stumbled upon your blog, so let me begin by saying that I am very grateful to read the thoughts of a surgeon who clearly cares very much about providing the best, and sometimes newest treatments for his patients. I am currently an undergrad at the University of Southern California and I am very interested in pursuing a career in surgery, particularly orthopedics.
So as for your post, I have a few questions regarding knee replacement surgery. You mentioned in your post that in a traditional replacement, the knee is aligned with its axis perpendicular to a line running from hip to ankle. Is a normal knee not always aligned like this? As far as I understood, this is the driving concept behind the Otis Med system, but it seems to me that most knees ought to be pretty close to this ideal that is used in the traditional replacement. In other words, is “customization” really worth the two or three degrees that a patient’s knee may be off by? As you said, the majority of traditional knee replacements can be expected to last several decades.Additionally, why is it that the Otis Med system looks at the degenerated knee and tries to reconstruct it to pick a replacement? Wouldn't it be easier to look at the healthy knee and assume symmetry? That way, no computer reconstruction would be necessary.
Forgive me if my comments seem uninformed or off-base. This is all very interesting to me, so I'm just trying to understand as much as I can.
Thanks,
JDM
“Are surgeries done through small incisions better?”
Comment:
Dr. Cluett,
This is a topic that has interested me for quite some time now. It seems to me that surgeons are constantly on the look out for ways to do less and less invasive surgery. In fact, I have even read about natural-orifice surgeries being performed on patients who really don't want scars. But what intrigues me the most is that often times these minimally invasive surgeries (particularly orthopedic ones, it seems) are very difficult for surgeons to perform, and thus increase the risk of surgical error. Do you think that this is indeed the case? Take, for example, a mini-hip replacement. I have read that there is concern about the ultimate alignment of the prosthesis with this technique.
Other minimally invasive surgeries, though, I feel are done because of a greater understanding of human anatomy. The Quad-sparing knee replacement provides an excellent. This procedure works around the quadriceps instead of through it so that the new joint can be better stabilized post-op. I think that it should be reasons like this, not cosmetic ones, that lead surgeons to create new surgical techniques. Thoughts?
Subscribe to:
Comments (Atom)
